Anatomy of the L4-L5 Spinal Motion Segment
Lowest spine vertebrae are the L4 and L5. The L4-L5 spinal part, as well as the intervertebral disc, soft tissues, nerves, joints perform different functions, for example, they support the upper body and move the body in different ways.
The L4-L5 segment carries a huge load and is characterized with flexibility, thus, unlike other lumbar segments, it is likely to be vulnerable to the injuries and/or regressive changes.
The L4-L5 motion segment consists of the following units:
- L4 and L5 vertebrae. Each vertebra has a vertebral body in front and a vertebral arch at the back. The vertebral arch has 3 bony apophysis: a spinous process in the middle and two transverse processes on both sides. So-called lamina is located between the spinous and the transverse processes. We use the word "pedicle" to describe the region between the transverse process and the vertebral body. Facet joints link the vertebrae, articulating cartilage wrapping these joints contribute into smooth motions between the neighboring surfaces.
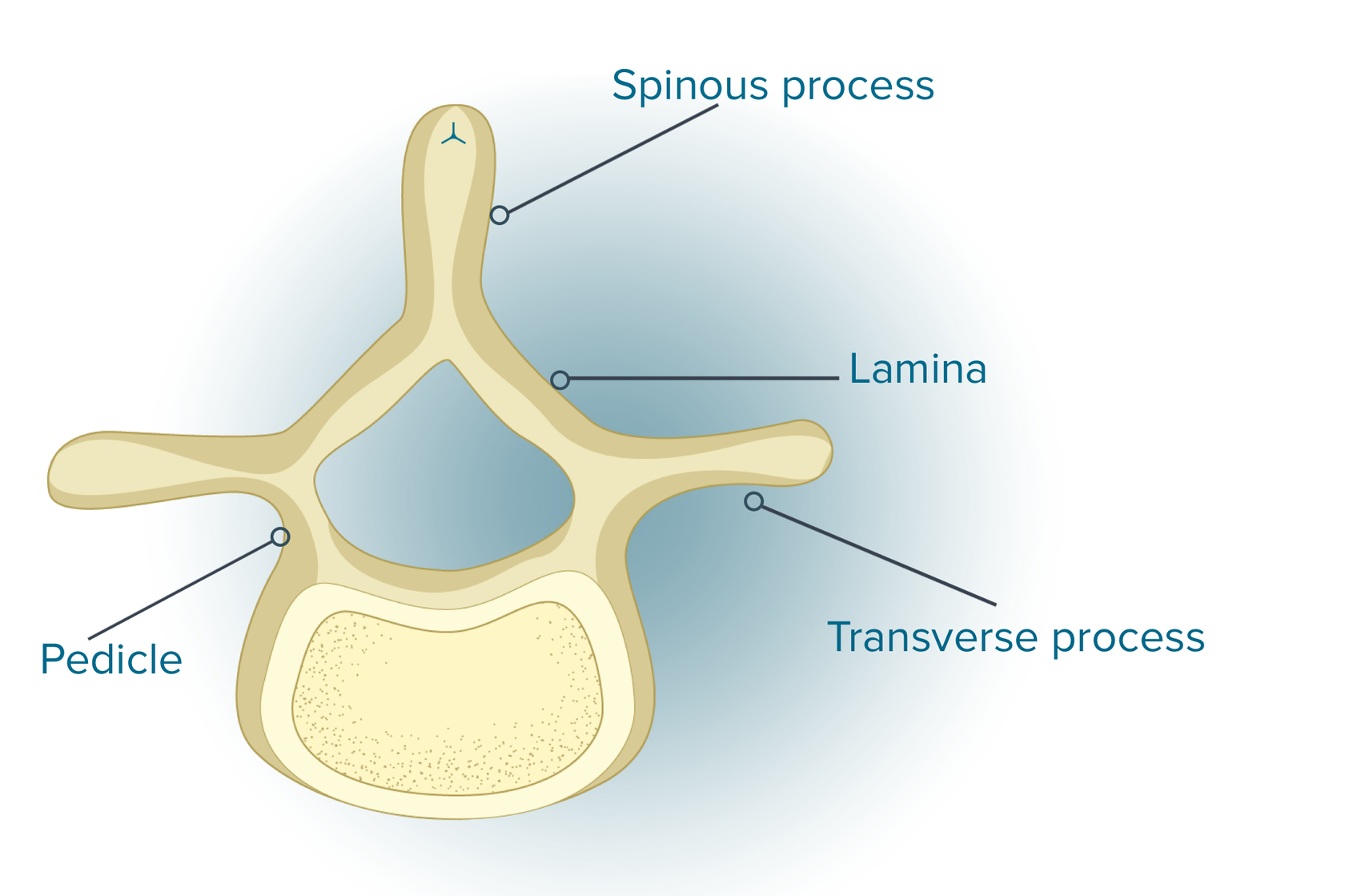
The frontal part of the L4 and L5 vertebral bodies is taller that their back part. Bony endplates which cushion the weight on the spine can be found on the upper and lower ends of each vertebral body.
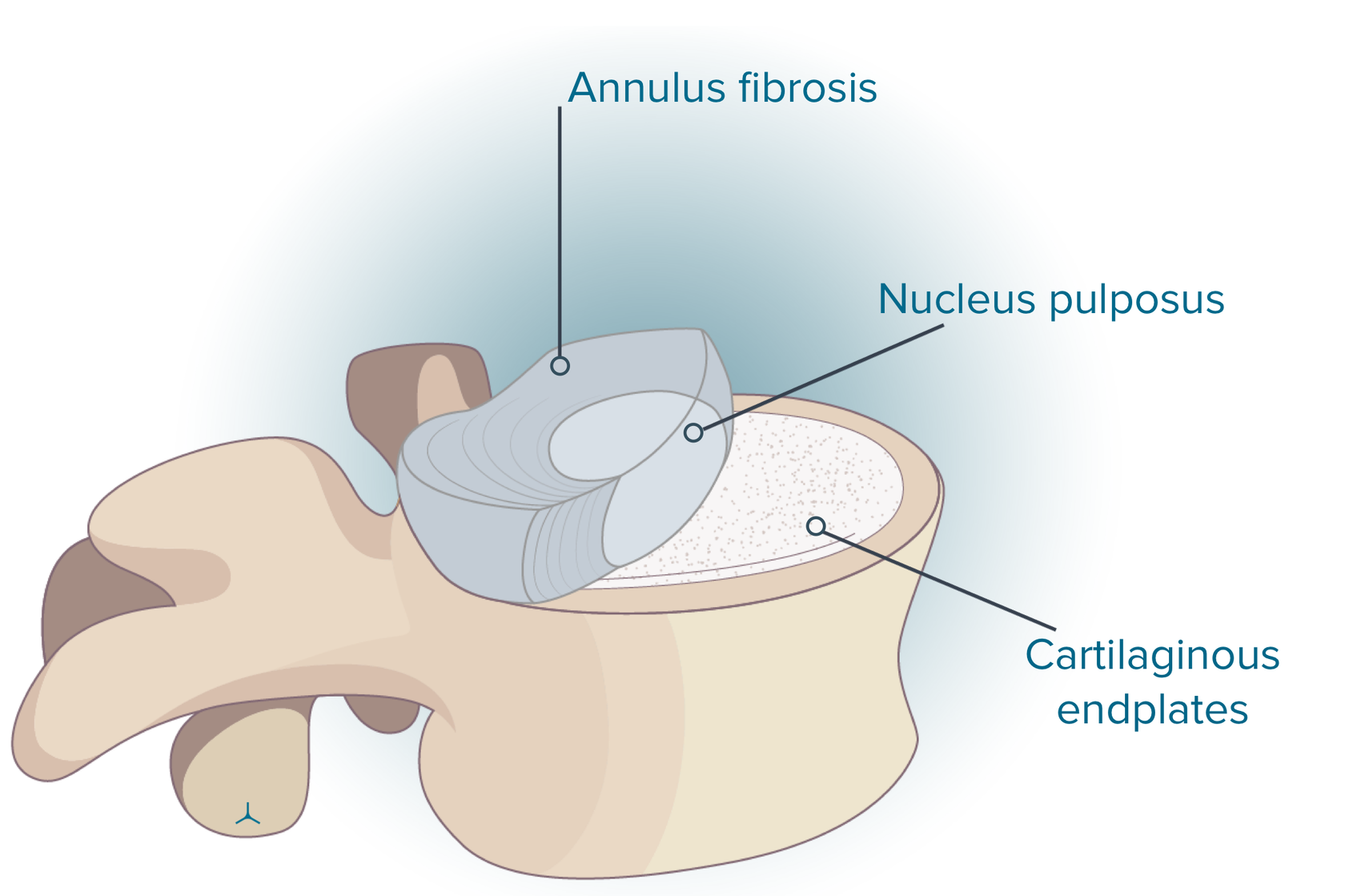
- L4-L5 intervertebral disc. The disc has three parts:
- Nucleus pulposus or the central part of the disc. Undamaged disc nuclei consist of nearly 77% water. The nucleus evenly distributes the load applied to the disc and removes pressure outward.
- Annulus fibrosis or the disc’s outer side with overlapping ligaments. The annulus wraps the nucleus and provides rupture-less movements in different directions due to its flexibility.
- Cartilaginous endplates or two pieces of cartilage that glue the upper and lower surfaces of the disc to the round, even area of each closest vertebrae. The disc endplates contribute into healthy discs because they serve to be the gatekeepers for nourishing substances and water to enter the disc region.
The intervertebral disc acts as follows:
- Spacer. The disc is high so that joints, muscles, and nerves have enough space for their adequate work. Each spinal segment includes a pair of vertebrae with the disc between them, and this unit functions as a motion joint.
- Shock absorber. The discs cushion the pressure exerted on the spinal column.
- Motion unit. The discs are flexible enough to move forward, backward, side to side, and rotate, they also support the spine and keep it upright.
Common Problems at L4-L5
The L4-L5 motion segment is characterized with the following more common injuries and disorders:
- Facet joint problems. The L4-L5 motion segment with its high mobility is susceptible to the disorders associated with the facet joints, such as osteoarthritis, synovial cyst (fluid-filled sac) formation, and facet instability.
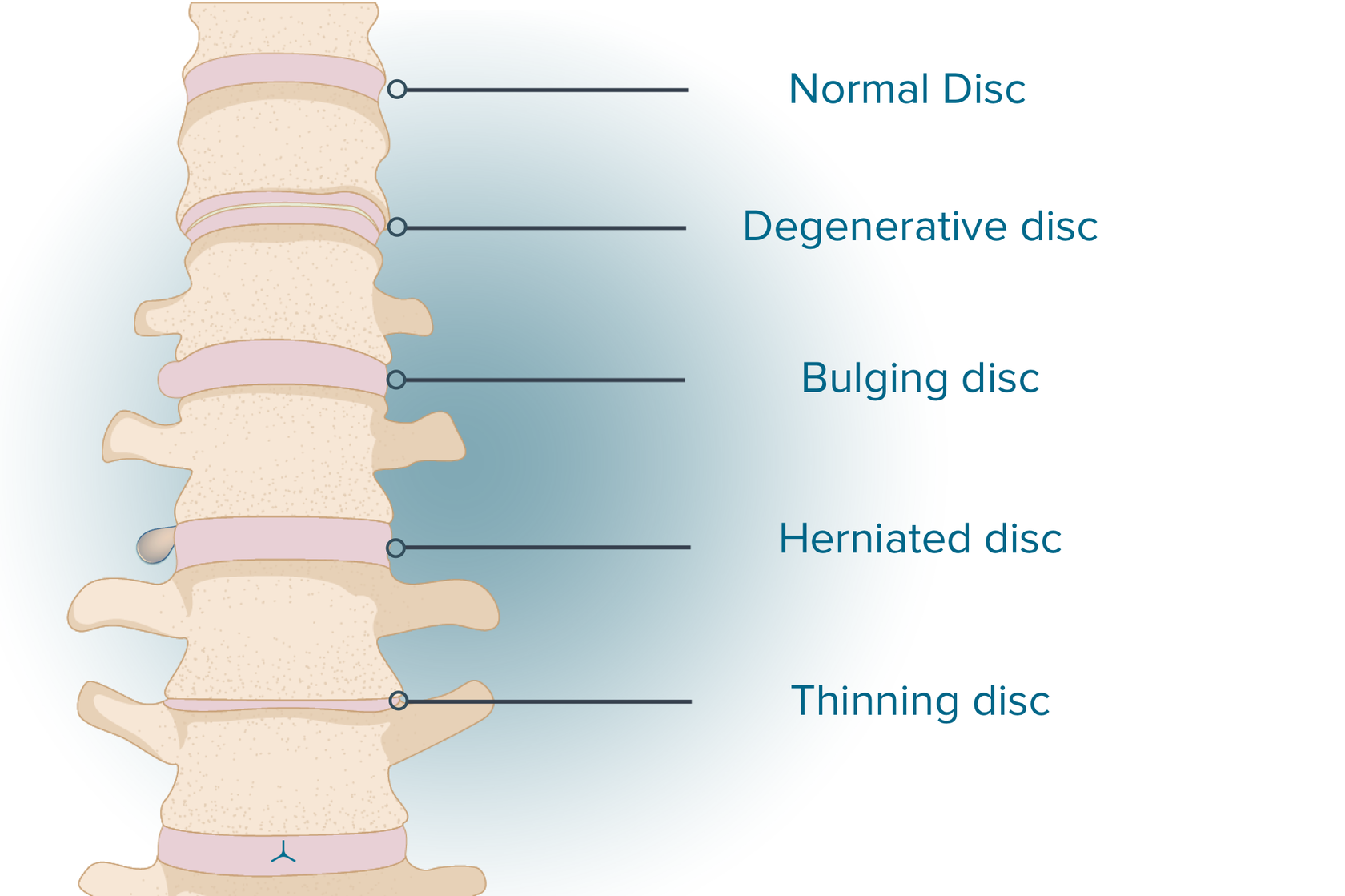
- Disc problems. Disc degeneration is a wide spread complication for the L4-L5 segment. This condition is likely to arise from the excessive loads at the L4-L5 motion segment and insufficient mobility in the segments below. Degeneration-induced change in disc height could damage the lordosis of the lumbar spine. Degeneration or injury could cause a hernia (90%-95% of all herniated discs occur in the segments where l4 l5 and s1 are located).A bulging disc is typical for the first stage of future protrusion/ herniation.
- Spondylolysis. Pars interarticularis (a small segment of bone from the vertebral arch joining the facet joints) is likely to fracture at the L4-L5 level because of the focused compressive loads in this region. It can happen on one or both sides.
- Degenerative spondylolisthesis. The L4-L5 facet joint changes are age driven, which makes it vulnerable to spondylolisthesis (forward slippage of L4 on L5) because of degenerative changes.
- Spinal stenosis. Narrowing (stenosis) of bony openings for nerves due to the bone spurs (atypical bone growth) or other degenerative changes is likely to result in compression of the nerve roots in the region of stenosis.
Outer trauma, including falls or motor vehicle accidents, may be the cause of facet joint dislocation, fracture, and/or damage to the cauda equina. The L4-L5 vertebrae and spinal segment rarely suffer from tumors and infections.
What is a Bulging Disc L4/L5?
What is l4 l5 disc bulge? A bulging disc could be observed in case the disc is displaced from its normal position and starts to occupy the space of spinal nerves. Literature describes different types of bulging discs with some of them bringing more pain than others. Actually, there is a wide variety of bulging discs, and even some people never know they have one, while other people suffer from so much pain that it lowers their quality of life.
The nucleus presses against the annulus, thus the disc starts to bulge or prolapse outward. The annulus still contained the bulged disc material. They can be symmetrical (along the entire contour of the disc) or asymmetrical, they are asymptomatic in many cases.
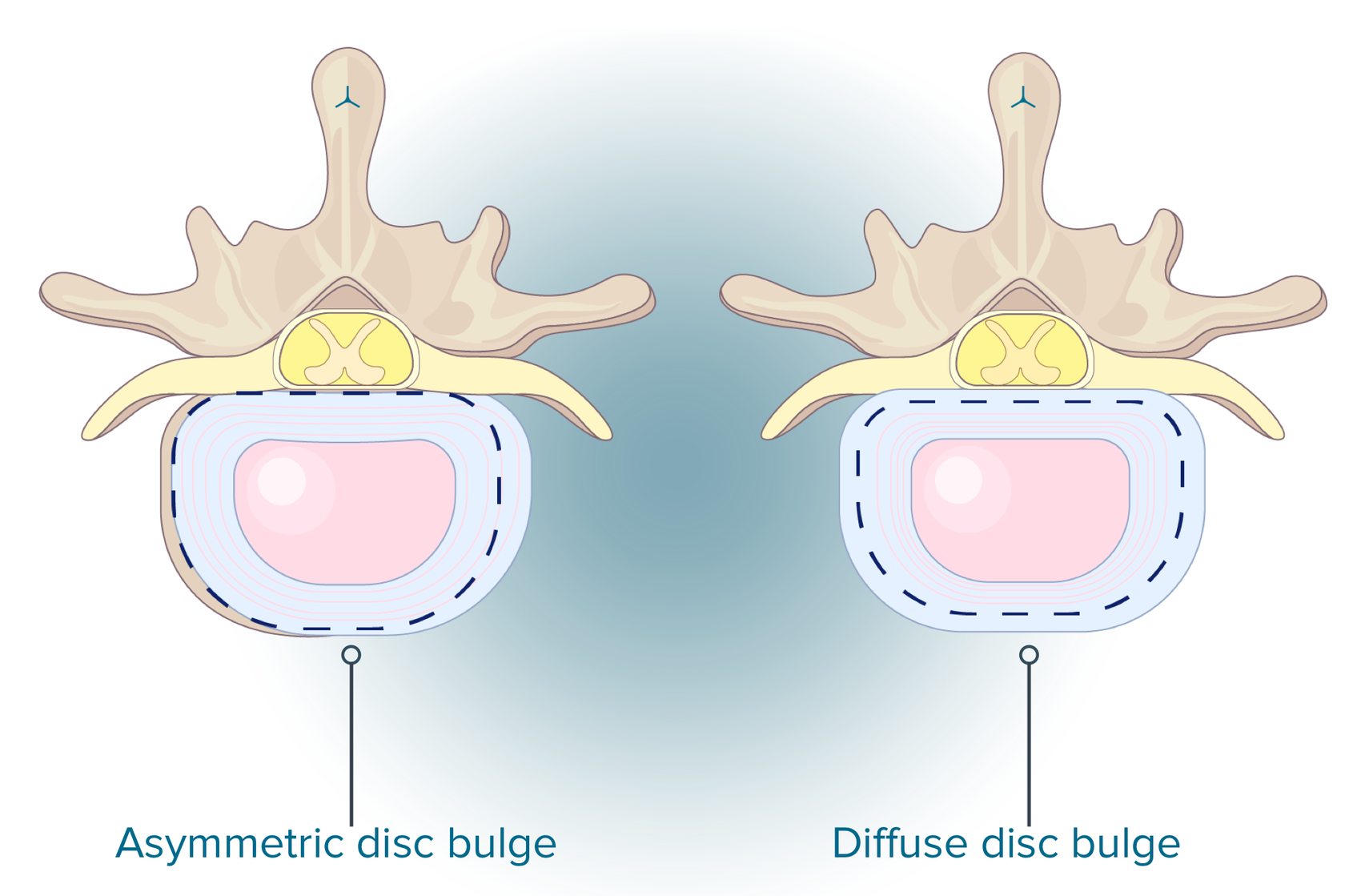
А) Asymmetric disc bulge (Broad-based disc bulge): The bulge occupies 25 to 50% of the disc.
В) Circumferential disc bulge (Diffuse disc bulge): The bulge goes beyond the entire disc circumference.
What is the Difference Between a Bulged Disc and Herniated Disc
A bulging disc protrudes beyond the space it would typically be located in. A larger part of the disc is affected by the bulging which extends at the hard outer layer cartilage. A bulging disc is seen to be a natural aging process, although it could be characterized by the different degrees of severity. If a crack in the hard cartilage causes the inner soft tissue to come out, it is called a herniated disc. This type of spinal disc is highly likely to cause pain, but just like a bulging disc, in many cases, they don’t.
What Causes A Bulging Disc?
Aging is the most popular reason for bulging discs. This occurs over time due to the water loss in the discs. A lack of water makes them stiffer, flatter, and in general more vulnerable to damages. Besides aging, any kind of insignificant trauma carries a risk of causing a bulging disc. Minor trauma exerts pressure on the internal soft core of the disk, stretches the outer layer, thus making it difficult to take its original shape. Patients with a bulging disc due to other reasons but aging are the ones who:
- Perform repetitive lifting, bending, driving, and standing
- Apply improper lifting techniques
- Used to play contact sports or be into extreme sport activities
- Have spinal disc problems in their family
- Have been in a car accident or suffered any kind of severe trauma
- Excessively drink or smoke
- Have poor posture
Common Symptoms of a Bulging Disc L4/L5
Bulging disc is manifested with many symptoms which depend on the spinal regions affected by it. As we’ve already said, it may happen so that bulging disc is not revealed in the symptoms. More often than not, people suffer from some kind of pain, weakness of the muscles, or numbness in the area of the bulge. They describe their abnormal sensations, such as a feeling of pins-and-needles and/or tingling. Men are more likely to be in the risk group for bulging discs which are also common practices with age.
If you observe the symptoms of a bulging disc in the neck, you will most likely experience pain, tingling, numbness, and weakness in the neck area. Sometimes these sensations may even radiate to other parts of your body, including your shoulders, arms, hands, and fingers.
About 90% of bulging discs occur in the lower back. Very often, bulging disc will be observed between your L4 and L5 vertebrae, and between your L5 and S1 vertebrae. Bulging disc in this region applies pressure on lower body spinal nerve roots. A bulging disc in the back is manifested by the pain in the pelvic region, legs, buttocks, and feet. These symptoms may be associated with the sciatic nerve.
Nonsurgical Treatment for a Bulging Disc L4/L5
If you search the Internet, you will be exposed to thousands of articles how to treat l4 l5 back pain. You will find a whole range of various options for l4 l5 pain treatment and how to fix a bulging disc l4 l5. All in all, treatment methods cover back bracing, medications, chiropractic, physical therapy, observing an anti-inflammatory diet, injections, and surgery may be recommended in some cases only. The first line treatments are to adjust your posture and to stick to the preventative measures.Here are the most popular Nonsurgical treatments of the L4-L5 Bulging Disc:
- Medication. The first medications to try are non-steroidal anti-inflammatory drugs (NSAIDs). If you experience severe pain, you might consider opioids, tramadol, and/or corticosteroids.
- Physical Therapy. If you suffer from difficult movement, a physical therapist might be of assistance in your recovery. Physical therapist can recommend special stretches and exercises aimed to expend your range of movements.
- Chiropractor. Chiropractors will identify the type of bulging disc you’re suffering from and even the causes of this condition. Chiropractors are trying to realign the spine as a treatment option.
- Anti-Inflammatory Diet. High levels of inflammation will adversely affect your bones, muscles, and joints. If you are at risk of going through an inflammatory process, you are more likely to handle bulging disc problems. In this case, your diet should include leaf green veggies, coconut oil, and olive oil.
- From our point of view the above-mentioned measures are out of place in many cases. From our side we recommend the next:
- Self-care. To support recovery process and/or prevent an L4-L5 injury from deterioration, it is recommended to avoid:
- Repeated bending of the spine
- Sudden, abrupt movements, such as jumping
- High-intensity exercise and lifting heavy weights
- Acupuncture — this method contributes into regeneration processes
- Physiotherapy -procedures can be different (Laser Therapy and Magnetic Therapy are the best ones as we see it). Beneficial procedures are highly recommended to the patients with many disorders in their medical history. One random procedure is definitely not be the reason for a significant relief, while repetitive physiotherapy could bring positive dynamics
- Therapeutic exercise.Well-balanced training of patients with physical exercises is one of the typical features of exercise therapy. Being fit is known to be a long-term unstopped process when the results of the previous training sessions could contribute into the next sessions. Regular physical exercises upgrade the fundamental functions. It is highly advised to follow method with the support from an expert trainer.
- Walking -this type of physical activity should be considered separately. The treatment goal is to improve disc metabolism. The vertebral disc has no vessels. They run through the vertebral body and their branches come close to the disc, and then diffusion helps nutrients and metabolic products penetrate the disc. To make diffusion successful, one needs to walk. At least five km a day is a good sign of your activity.
Please don’t forget that the best way to prevent future l4 l5 disc herniation is to prevent the disc bulging/protrusion.
Surgical Treatment for L4-L5 Bulging Disc
Surgical methods of treatment for this pathology should be carried over for consideration in extreme cases. It has to be said that here we are not talking about traditional surgical treatment.
Among the methods:
- block Injections, which help to reduce pain along the course of the nerve root.
- puncture surgical methods of treatment. It is made with a puncture needle in the direction of pathological bulging disc (protrusion) and with the help of special drugs or radiofrequency exposure. After the procedure the pressure in the intervertebral disc is reduced, which makes it possible for disc to take its original shape. In this case, the nucleus pulposus in the center between the bodies of the two vertebrae is subject to partial destruction by cold plasma, laser or electromagnetic waves.
Such surgical treatment refers to minimally invasive procedures and is carried out most often under local anesthesia. The recovery period is quite short and does not require much effort from the patient.
